There is a point at which a health crisis stops being about medicine and starts being about power.
Black maternal health in the United States has reached that point..again.
The data has been clear for years. Black women are far more likely to die during pregnancy and childbirth than their White counterparts. Even as maternal mortality declined overall in 2023, Black women continued to die at rates more than three times higher than White women: 50.3 versus 14.5 per 100,000 birthsThe gap persists across income and education levels. A college-educated Black woman is still more likely to die in childbirth than a White woman without a high school diploma.
At this stage, it cannot be explained away by socioeconomic status. Black women with higher incomes and advanced degrees still face worse outcomes than White women with fewer resources. The disparity holds across education levels, insurance status, and access to care.
This is not about individual behavior or circumstance.
It is structural.
And increasingly, it is paired with something else:
Control.
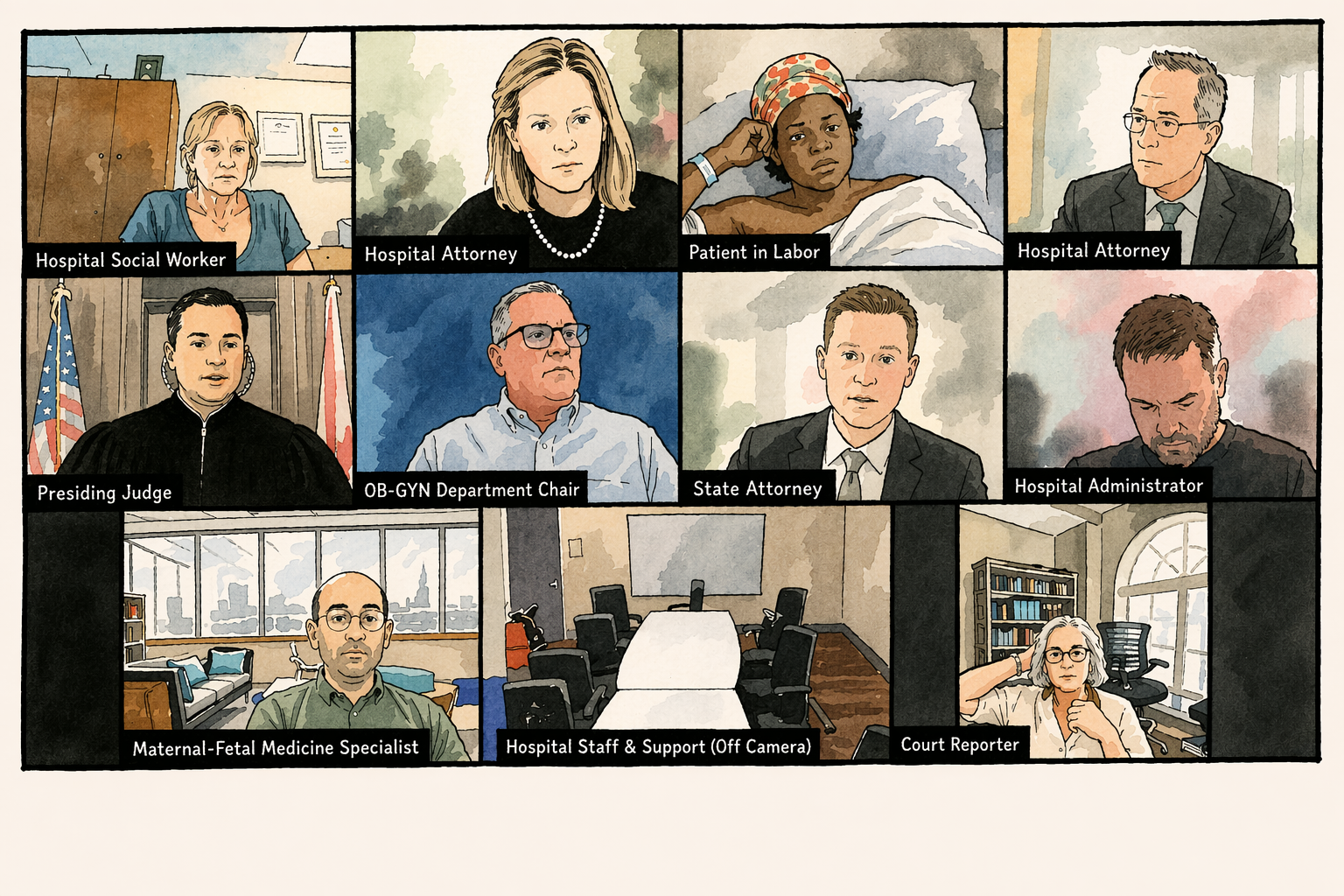
When a Delivery Room Becomes a Courtroom
Cherise Doyley arrived at a Florida hospital in labor with a plan.
A mother of three and trained doula, she understood both the risks and variability of childbirth. After prior C-sections, doctors recommended another surgical delivery due to the risk of uterine rupture. She acknowledged the risk, understood it to be relatively low, and chose to attempt a vaginal birth.
For several hours, she labored.
Then, without warning, a tablet was brought to her bedside. She was placed in a virtual court hearing while still in labor. Without legal representation or a patient advocate, she was asked to defend her decision before a judge, hospital attorneys, and clinicians.
The discussion centered on risk to the baby. Far less attention was given to the risks she faced—risks she knew personally, including complications and hemorrhage from prior surgeries. She raised concerns about recovery, about caring for her children, and about the possibility of dying.
After more than two hours, the court ruled that the hospital could proceed without her consent if conditions worsened.
Hours later, following concerns about the baby’s heart rate, she underwent a C-section.
She was brought back into another hearing shortly after…before she had even seen her newborn.
Why Are Courts Involved at All?
Outside of pregnancy, a competent adult has the right to refuse medical treatment. Yes, even if that refusal carries risk. Both the mother and the baby matter. That should be the baseline. The mother is not a variable in a theoretical equation. She is a living, breathing person with agency, history, and a life that extends far beyond the moment of birth.
When everything is filtered through the singular lens of “saving the baby,” the mother’s role begins to erode—not explicitly, but functionally. Her voice carries less weight. Her preferences become negotiable. Her body becomes the vessel through which an outcome is achieved, rather than something to be protected in its own right.
A child does not arrive into the world in a vacuum. A child is born into a life—one shaped by the health, presence, and wellbeing of their mother. When those elements are compromised, the impact is lasting and does not end at birth. It extends into everything that follows.
And in a country that struggles to support mothers after delivery through fragmented care, limited leave, and uneven access to resources, the emphasis on preserving the pregnancy at all costs begins to less protective and more nefarious. It raises a much harder question:
Are we supporting lives—or just preserving bodies?
This Is Not New—It’s A Pattern
Modern gynecology was built, in part, through experimentation on enslaved Black women by physicians such as J. Marion Sims, who performed repeated surgical procedures without anesthesia. In the 20th century, the Tuskegee Syphilis Study withheld treatment from Black men for decades, even after a cure became available.
These were not isolated events. They established a precedent: that Black bodies could be overridden in the name of science, safety, or progress.
That precedent has not disappeared. It has evolved.
Today, it appears in more subtle, yet equally consequential ways. Black women are more likely to have their pain dismissed, their symptoms minimized, and to experience delays in treatment. High-profile cases such as Serena Williams nearly dying after childbirth when her concerns about a blood clot were initially ignored underscore that status and visibility do not eliminate risk.
Doyley’s case fits within this continuum. What begins as medical concern can escalate into enforcement. A disagreement becomes a legal matter. A patient becomes subject to decision-making rather than the source and driver of it.
Control, Framed as Protection
Cases like this are often presented as “exceptional,” “urgent,” “necessary,” “in the best interest of the child.”
But they function as something else entirely. They are tests.
They reveal how far institutions can go in asserting control over women’s bodies, particularly Black women’s bodies, while framing that control as protection.
“We’re trying to save the baby” becomes the justification wielded as an impenetrable shield.
Black women are often the first to experience these boundaries being pushed. That pattern is not incidental. It’s predictive.
What is tolerated there becomes the standard. Once that precedent is set, the line has already moved.
At the Same Time: A Declining Birth Rate
While these dynamics unfold, the United States is facing declining birth rates. There is growing concern about fewer people choosing to have children. But, there is a disconnect between that concern and the conditions being created.
The U.S. remains one of the only high-income countries without universal healthcare or guaranteed paid maternity (nor paternity) leave. Maternal care is fragmented. Costs are high. Outcomes are inequitable.
Women are not opting out of motherhood because they do not understand its value. They are making decisions based on what they observe.
- Risk to their bodies
- Risk to their autonomy
- Risk to their long-term health
When those risks include the possibility that their medical decisions could be challenged or overridden, the calculation changes. It becomes a huge, “no, thank you.”
What This Moment Reveals
If the goal is safer pregnancies and stronger families, the solution is not the erosion of rights.
It is trust. It is respecting informed refusal, improving quality of care, addressing bias directly, and ensuring that no woman has to defend her autonomy while in labor.
Because at its core, this is not only about health. It is about who is allowed to decide.
Cherise Doyley entered a hospital to give birth and instead found herself in court during what should have been one of the most sacred and protected moments of her life.
Black women are navigating systems that have long treated their autonomy as negotiable. The difference today is ease of visibility. We can see it as it unfolds in real time.
The question now is whether we will allow the courts to overreach into our rights as patients. Are we paying attention? Because prevention is far less costly than undoing the legal erosion of bodily autonomy.
References
Centers for Disease Control and Prevention. (2025). Maternal mortality rates in the United States, 2023.
Kaiser Family Foundation. (2025). Racial disparities in maternal and infant health.
March of Dimes. (2024). Maternal mortality and racial disparities report.
Yurkanin, A. (2026). She was in labor at a Florida hospital. Then she was in Zoom court for refusing a C-section. ProPublica. Yurkanin, A. (2026). They didn’t want to have C-sections. A judge would decide how they gave birth. ProPublica.
American College of Obstetricians and Gynecologists. (2020). Refusal of medically recommended treatment during pregnancy. Washington, H. A. (2006). Medical apartheid.
Jones, J. H. (1993). Bad blood: The Tuskegee syphilis experiment.
World Health Organization. (2023). Maternal mortality: Global health estimates.
Farber, S. (2018). Serena Williams on childbirth, postpartum complications and making a comeback. The New York Times.




Leave a Reply